Parkinson’s Disease and Dyskinesia
If you have Parkinson’s disease (PD), there is a good chance that you’ve been, or will be taking medication containing levodopa. Levodopa is administered in combination with the drug carbidopa. This drug combination is considered standard treatment for PD symptoms such as tremor, muscle stiffness, and slowness of movement. Taking levodopa however, is associated with a side effect called dyskinesias. Learn more about dyskinesia, what causes it, how it can be managed, and some basic coping strategies below.
What is dyskinesia?
The features of dyskinesia include rapid, involuntary, and uncontrollable movements other than tremor that can present as body swaying, writhing, twisting, squirming, flailing, fidgeting, or bobbing. Dyskinesia initially appears on the side of the body worst affected by PD. Although it can be localized to one part of the body such as the legs and arms, it can also spread to the torso, head, neck, and face. In some circumstances, dyskinesia can also affect speech as well as respiratory and eye muscles.
What causes dyskinesia?
Taking dopaminergic medication like levodopa may lead to the development of dyskinesias. However, taking these medications early on in the disease does not usually result in dyskinesias. Dyskinisias tend to occur in people who are taking levodopa who also have more neurodegeneration in the brain, that is, when the disease has progressed. It is less likely in people taking levodopa who are in earlier stages of PD.
The underlying cause of dyskinesia is complex and is not completely known. Normal brain function depends on a complex network of cells that communicates and functions via an array of different brain chemicals. One of these chemicals is dopamine. In PD, there is a loss of brain cells called dopaminergic neurons that make dopamine; therefore, the level of dopamine in the brain starts to decrease.
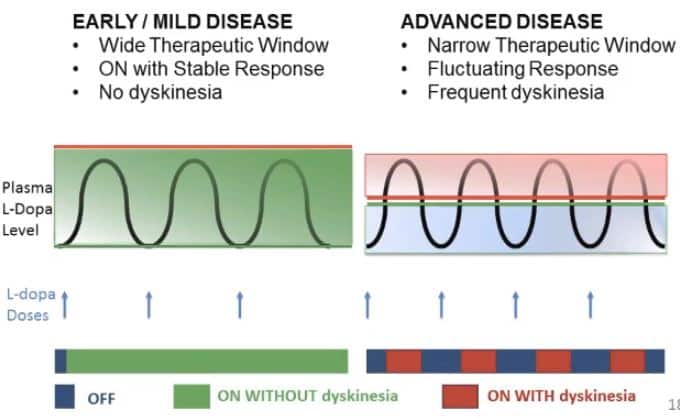
The purpose of taking levodopa is to temporarily restore the dopamine that is lost. However, since levodopa is intermittently taken over the course of a day, the level of dopamine will rise and fall. These dopamine level fluctuations, in combination with the loss of dopaminergic neurons, are thought to cause dyskinesia. Dyskinesia can occur when the level of levodopa in the body is at a maximum, referred to as peak dose dyskinesia, or when the levels of levodopa are rising or falling, referred to as diphasic dyskinesia.
If levodopa causes dyskinesia, then why should I take it?
At present, treatment with levodopa is the most effective way to relieve tremor, stiffness, and slow movement associated with PD. Although in the early stage of PD, levodopa may not be necessary and there are other medications available to treat this stage of the disease, as the disease progresses and its symptoms interfere with daily living, your doctor will most likely prescribe levodopa to improve your quality of life.
Who gets dyskinesia?
Being diagnosed with PD at a younger age (less than 50, also known as early onset PD or young onset PD) is associated with a greater chance of developing dyskinesia.
Are there resources to learn more about dyskinesia?
APDA provides information, education, and support to those impacted by Parkinson’s disease and has a full library of resources on all PD-related topics.
Check out our resources about levodopa and dyskinesia that may be helpful:
- APDA funding is critical to new research in understanding Levodopa-induced dyskinesias
- Understanding Dyskinesia: Spotlight on Parkinson’s Webinar

Watch Our Webinar: Spotlight on Dyskinesia and Off – Feeling Good Every Day
Speaker: Rebecca Gilbert, MD, PhD
Vice President, Chief Scientific Officer
American Parkinson Disease Association
Are there ways to manage dyskinesia?
Development of dyskinesias requires two things:
- the person with PD needs to be taking levodopa
- there needs to be a certain level of neurodegeneration in the brain
This means that if you start taking levodopa and it causes dyskinesias that are bothersome, you can lower or stop levodopa (with your doctor’s guidance) and the dyskinesias should resolve. This also means that the clock to developing dyskinesias does not start when you start levodopa. It starts when the disease starts. Therefore, delaying levodopa until later in the disease and then starting levodopa later will not prevent dyskinesias. It just means that there will be a shorter lag time between starting levodopa and developing dyskinesias.
Here are some additional strategies to manage dyskinesias:
- It is important to note that mild dyskinesia may not be bothersome, and the mobility afforded by taking levodopa may be preferable to the immobility associated with not taking levodopa. People with PD must weigh the benefits of using levodopa versus the impact of dyskinesia on their quality of life. If dyskinesia is not bothersome, you can choose to remain mildly dyskinetic on your current dose of medication in order to retain the benefits of your current dose of medication.
- If you have dyskinesia that is interfering with your daily life, your doctor may lower the dosage, adjust the time at which carbidopa-levodopa is taken, prescribe an extended-release formulation of this drug combination (such as Rytary® or Crexont®), or recommend continuous intestinal infusion of carbidopa/levodopa (Duopa™) or continuous subcutaneous infusion of foscarbidopa/foslevodopa (Vyalev™). These treatment strategies may help reduce fluctuations in dopamine that contribute to dyskinesia. (See APDA’s Approved Medications for Parkinson’s Disease for a full list of PD-related medications.)
- The drug amantadine can reduce dyskinesia and can also help PD symptoms. Amantadine (Symmetrel®) can be taken in multiple daily doses, or in an extended-release formulation (Gocovri™) that maintains a high level of amantadine in the body throughout the day and has shown good results in reducing dyskinesia. In addition, the extended-release formulation taken orally – once at bedtime – may be more advantageous to some people than the multiple daily doses of immediate-release amantadine.
- Deep brain stimulation (DBS) is a surgical method that can be used to manage PD symptoms and dyskinesias. It can be very effective in carefully selected patients. Focused ultrasound (FUS) is another procedure that can be effective for these issues.
Are there coping strategies for living with dyskinesia?
There are several ways to manage dyskinesia and PD in general by incorporating some basic routines into your lifestyle.
- Keep a diary that logs the time and frequency of dyskinesia, which will help your doctor assess if your medications are working and help you schedule daily activities when mobility is better. The APDA Symptom Tracker app can help you keep track of a wide range of motor and non-motor PD symptoms, including dyskinesia.
- Physical activity, including mild aerobic exercise such as walking, dancing, and swimming, will help keep the body strong and prevent muscle weakening. APDA has virtual exercise and movement classes for you to explore.
- Stress can make dyskinesia symptoms worse, so find ways to reduce stress (breathing exercises, massage, yoga, etc) and try to keep a positive attitude. Creative activities can also be beneficial physically, mentally, and socially.
- Poor sleep at night is associated with dyskinesia. Aim for good sleep quality and try to experiment with different positions in bed that will help you relax and sleep better.
Explore Our Parkinson’s Resource Library
Whether you are living with PD, caring for someone with PD, or are just looking for information, check out our new resource library to see articles, videos, webinars, and more in-depth information about Parkinson’s disease.