DaTscan: A test to help in the diagnosis of Parkinson’s
What is a DaTscan and how is it performed?
In 2011, the Food and Drug Administration (FDA) approved an imaging test to help diagnose Parkinson’s disease (PD) called DaTscan (dopamine transporter scan). In this test, a radioactive tracer, Ioflupane (123I), also known as DaTscan, is injected into the blood, where it circulates around the body and makes its way into the brain. It attaches itself to the dopamine transporter, a molecule found on dopamine neurons. Several hours after the tracer has been injected, special imaging equipment scans the head to detect the presence of DaTscan.
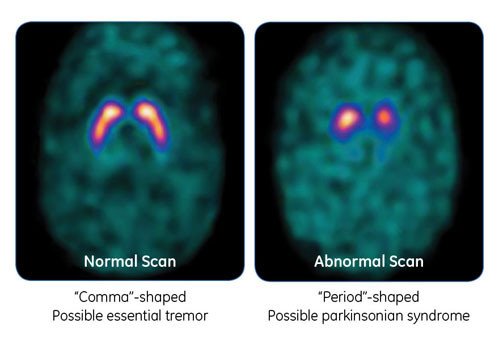
People with PD will typically have a smaller signal in a part of the brain called the striatum, where the ends of the dopamine neurons are meant to be. Here is a normal scan on the left, which would indicate a healthy dopamine system, next to an abnormal scan on the right, which would indicate an unhealthy dopamine system.
It is important to note that conventional MRI imaging will appear normal in PD and is therefore not helpful in confirming the diagnosis. Other atypical parkinsonian conditions, such as vascular parkinsonism however, can have abnormalities on MRI, so the test may be done to rule out other diagnoses.
How accurate is a DaTscan?
Stated plainly, once the motor symptoms of PD are evident, diagnosis of Parkinson’s via DaTscan and clinical exam are similarly accurate. In most cases, PD can be correctly diagnosed by clinical exam since there are many characteristic features of PD that can be easily elicited. Therefore, despite the DaTscan being available to help diagnose Parkinson’s, in most clinical situations, a DaTscan will not add information to what can be gleaned from the clinical exam. One study actually demonstrated that the accuracy of diagnosis in early PD was the same whether the diagnosis was reached using clinical exam or using DaTscan.
What are the pitfalls of DaTscan?
DaTscan will appear abnormal in any disease in which there is a loss of dopamine nerve endings in the striatum. Therefore, Parkinson-plus syndromes, discussed in a prior blog, such as Progressive supranuclear palsy (PSP), Corticobasal ganglionic degeneration (CBGD), and Multiple system atrophy (MSA) all typically demonstrate abnormal DaTscans. DaTscan therefore cannot be used to distinguish between these syndromes.
Every medical test (for any disease) has a false positive and a false negative rate. This means, that it is inevitable that in a certain (small) percentage of people who have PD, the DaTscan will be read as normal and in a certain (small) percentage of people without PD, the DaTscan will be read as abnormal. Results of any medical test that is performed, must therefore be considered within the entire clinical context.
When is DaTscan helpful?
There are situations in which DaTscan can be very helpful in securing a diagnosis – when neurologic exam findings are not clear-cut. Although DaTscan cannot distinguish PSP, CBGD, and MSA from PD, studies suggest that it may be able to distinguish drug-induced parkinsonism and vascular parkinsonism from PD.
The FDA indication for DaTscan is for distinguishing between PD and essential tremor (ET). Usually it is quite straightforward for a neurologist to distinguish between the tremors of ET and the tremors of PD. PD tremors occur at rest and are accompanied by slowness and stiffness of the limb, whereas ET tremors occur with action and are not accompanied by slowness and stiffness of the limb. However, some people may have mixed tremor features making the diagnosis more difficult. In those cases, a DaTscan can be very useful.
What are the limitations of the test?
Currently, DaTscan that is in clinical use is not quantitative, which means that the test is not designed to determine how impaired the dopamine system is – just whether it is or is not. This means that the test is not used to tell you whether the disease has progressed over time and is not used to follow a patient’s disease.
Is DaTscan abnormal before a person shows motor symptoms of Parkinson’s disease?
The short answer is yes. However, DaTscan is not used currently as a clinical test to screen for the disease before motor symptoms are evident. This may be changing, however. The PD scientific and research communities are now evaluating how the diagnosis of PD is made and efforts are underway to develop systems of PD diagnosis based on biomarkers, which are measurable characteristics in the body that indicate that disease is present, and not based solely on clinical symptoms.
In one biological staging system that is being proposed, researchers described a new pathologic condition that they named Neuronal synuclein disease (NSD). NSD is defined as disease states in which there are both dopaminergic neuron dysfunction/degeneration, detected by DaTscan, and abnormally aggregated alpha-synuclein, detected by lumbar puncture. Both of these biologic abnormalities can be present before motor symptoms of PD are evident, which means that in the future, disease may be diagnosed in the absence of motor symptoms. This is exciting to contemplate as it would allow people with very early disease to potentially be included in clinical trials. In addition, in the future, when medications that slow down the progression of PD are developed, they could be prescribed to people very early in their disease, hopefully preventing progression into full-blown PD.
How long does a DaTscan procedure take?
In total, a DaTscan can take 4-8 hours. The timeline breaks down as follows:
- 1 hour before the DaTscan injection, a drug is taken to reduce the thyroid’s accumulation of iodine 123.
- The DaTscan is injected intravenously into the arm.
- Then, there is a 3-6 hour waiting period while the DaTscan travels through the bloodstream and eventually into the brain.
- Finally, the scan itself takes about 30 minutes, with the doctor or technician using the scanning equipment to take pictures of the brain.
I’m told I have PD, but my doctor did not order a DaTscan – why not?
Many patients with PD are frustrated and sometimes frankly suspicious about how it is diagnosed. As a neurologist, over the years I’ve heard comments like:
- “All the doctor did was have me make some movements with my hands and legs and watch me walk and then he told me I had Parkinson’s disease! How is that possible?”
- “I don’t believe my diagnosis. Aren’t there a bunch of other diseases it could be?”
- “How can they know for sure? I want a test to prove whether I do or do not have Parkinson’s disease!”
Parkinson’s remains a clinical diagnosis
As mentioned above, there has been a lot of exciting news about the development of biomarkers for PD. And in the future, biomarker testing may revolutionize how PD is diagnosed, moving up the timeline to before the onset of motor symptoms. It will likely also change how early PD can be treated and how clinical trials for PD are run.
However, it remains the case, that once motor symptoms of PD are present, even subtle ones, it is typically very easy for a neurologist to diagnose PD. That is because many of the clinical features of PD are unique to PD and can be elicited via a neurologic exam in a doctor’s office.
Rest tremor for example, is seen in virtually no other illness. One skill of a neurologist is being able to distinguish a rest tremor from other tremors. While it is true that some people with PD do not have a rest tremor, which can make the diagnosis trickier, nevertheless, many elements of the standard in-office neurologic exam are very characteristic of PD, such as:
- decreased blink rate
- small handwriting, that decreases in size as the writing continues
- small, movements of the hands and the feet, worse on one side,
- characteristic stiffness of the arms and the legs, worse on one side,
- stooped posture
- decreased arm swing on one side while walking
- the characteristic walk in which the whole foot is planted flat at one time – instead of the heel being planted on the ground first
- the characteristic way of turning by taking multiple steps and not pivoting
If there are enough of these features present during an exam, with or without a rest tremor, especially if coupled with a history of certain non-motor symptoms that typically appear before the movement symptoms of PD, such as constipation, loss of smell and REM behavior sleep disorder, the practitioner will feel sure of the diagnosis.
It may seem like a brief exam, but all of the above can be assessed quickly. It is important to note, that a person who displays some of these features on exam may be unaware of them, while a trained neurologist can easily identify them. The converse is also true – a person may be very concerned that his/her symptoms are consistent with PD, while a trained neurologist can easily reassure the person that that is not the case.
The bottom line is that most people can be diagnosed with PD without any additional testing. However, as discussed above, when the clinical exam findings are not clear to the examiner, a DaTscan can be helpful and other biomarkers are currently being assessed for their usefulness in clinical practice.
Tips & Takeaways
- DaTscan is a test that can help in the diagnosis of PD, although in most situations a clinical exam done by a neurologist offers the same information.
- Neurologists are skilled in diagnosing PD through a clinical exam. While the exam to some may seem very basic and thus a PD diagnosis subjective or questionable, neurologists are well-trained to assess and diagnose (in most cases) with confidence.
- DaTscan may be useful in distinguishing PD from certain conditions, but not from others, so talk with your neurologist about whether DaTscan would be useful in your specific situation.
- DaTscan is not a test used for monitoring PD progression. It can be used to help clarify a PD diagnosis, but it is not a test you would undergo multiple times during the course of your disease.
- In the future, DaTscan may be used in combination with other testing to diagnose disease prior to the onset of the classic motor symptoms of PD.
Have a question about Parkinson’s disease?
Our Scientific & Medical Affairs Department can provide expertise and resources to answer your questions and address your concerns.